

3·
8 hours agoAnd actually burns up Harris votes in the process, making it even easier for him.
Fuckety fuck fuck.
And actually burns up Harris votes in the process, making it even easier for him.
Fuckety fuck fuck.
since Elizabeth was unlikely to have had her at much younger than 19.
Why? Because you think she would’ve got married earliest at 18 and never had sex before it?
She could’ve been fucking plenty and then gotten married when she got pregnant. And you don’t need to be that old to marry, and 100 years ago even less so.
In states without a legislated minimum, common law (which specifies a minimum of 12 years old for females and 14 years old for males) prevails; the estimated effect of a common law is similar to a legislated minimum of 13 or less
https://en.m.wikipedia.org/wiki/Marriage_age_in_the_United_States
Not just the fall of the Soviet Union.
The rise and fall of the Soviet Union.
What? I’ve been arguing squid for days in this thread.
Yes. Smoking causes increased mortality through increased rates of cancer, and smoking is thr most commonly used method of consuming cannabis.
That’s exactly what I’ve been saying, and you argued Squid as well, so I tagged you.
Now he’s ran from the convo, and a mod told me to drop it.
What I did drop is my respect towards squid
Fair enough.
Just really irks me when someone pretends like they “won” the debate while leaving.
“Don’t play chess with a pigeon. They will just shit on the board and knock over pieces.”
And it irks me because I really had faith in him, and now the blindly ignorant hypocrisy they’ve displayed here has basically ruined one of the biggest posters on Lemmy for me. Eh. Too bad.
Thanks for the warning instead of just banning, that’s some good modding. I respect that.
The lenghts you go to to avoid admitting you said/did something that might be considered silly.

That is the first reply you made. I then explained no-one is saying that cannabis is killing people — admittedly having forgot the mortality stat on the chart. The mortality stat doesn’t mean cannabis is “killing” people.
Then you start your inane sealioning, which you continue up until yesterday, at which point you blame me and @[email protected] of “not reading the study” and it “not having sources”, but you keep referring to Nutt’s study, when it cites it sources, which you clearly haven’t gone and read, which I’ve linked quite a few times now.
What I’m betting you did is read the cover of this link: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)61462-6/abstract saying “they don’t say where their numbers are from”. That’s like reading the back-cover of a murder mystery and saying “it’s dumb, they didn’t even resolve the whole murder!”
If you actually log in and read the FULL TEXT, you will see the data.
They source several different studies for different citations. I’ve done the work for you and here’s the most relevant ones.
They also explain just how they’ve weighed all the data:
During the decision conference participants assessed weights within each cluster of criteria. The criterion within a cluster judged to be associated with the largest swing weight was assigned an arbitrary score of 100. Then, each swing on the remaining criteria in the cluster was judged by the group compared with the 100 score, in terms of a ratio. For example, in the cluster of four criteria under the category physical harm to users, the swing weight for drug-related mortality was judged to be the largest difference of the four, so it was given a weight of 100. The group judged the next largest swing in harm to be in drug-specific mortality, which was 80% as great as for drug-related mortality, so it was given a weight of 80. Thus, the computer multiplied the scores for all the drugs on the drug-related mortality scale by 0·8, with the result that the weighted harm of heroin on this scale became 80 as compared with heroin’s score of 100 on drug-specific mortality. Next, the 100-weighted swings in each cluster were compared with each other, with the most harmful drug on the most harmful criterion to users compared with the most harmful drug on the most harmful criterion to others. The result of assessing these weights was that the units of harm on all scales were equated. A final normalisation preserved the ratios of all weights, but ensured that the weights on the criteria summed to 1·0. The weighting process enabled harm scores to be combined within any grouping simply by adding their weighted scores. Dodgson and colleagues3 provide further guidance on swing weighting. Scores and weights were input to the Hiview computer program, which calculated the weighted scores, provided displays of the results, and enabled sensitivity analyses to be done.
So no matter how much you want to sealion and pretend you weren’t wrong and didn’t say anything silly, I have offered you the data several times. And this all ignores the fact that you keep ADAMANTLY IGNORING a question I’ve put to you more than a dozen times; do you accept that a lot of cannabis use is SMOKING and that SMOKING causes increased mortality?
For one thing, they’re much better at googling than I am.

I’m literally showing you the very source of the statistics. Which you’re just refusing to accept, because presumably you’re incapable of going “oh, my mistake, I was wrong.”
That’s the scientists explaining — in detail — how the data was collected and where from. I also went into the sources of that study. Did you actually log into the Lancet and read the article, or open, see you need an account and go “oh whatever”?
You’ve several times now, asked “do you know the LD50 of cannabis” and “how exactly is cannabis killing people”. Straight up refusing to accept that I’ve explained in detail the difference between drug related and drug specific mortality and how both stats can have things in them without anyone having claimed that a person died of too much cannabis in their system.
Why do you keep ignoring the fact that people SMOKE cannabis and smoking causes a higher mortality rate? I said that before reading the studies, but now that I have done they also explicitly state that, like I KNEW they would.
Both of these quantify deaths from cannabis, but explicitly state the actual LD50 to be unknown, as there’s fewer than three reports of people having died and those can’t be ascertained to be because of cannabis. So they get the LD50 from animals and extrapolate it to humans based on fancy maths. And explicitly state that. Both of them give substances safety ratings. The rating for heroin is 6. Alcohol 10. MDMA 16. The study concludes that they show that MDMA’s dangers have been exaggerated, and it’s inline with cocaine and meth etc. The number for cannabis, you’re asking? They rate it as >1000.
No-one is claiming people are dying of cannabis overdoses, and now that we’re this deep in this thread, there’s no way you’re gonna back on that childish assumption. So I await more bullshit sealioning and excuses despite me linking the methods and sources of all the fucking data from the economist article that you pretend you were too incapable of Googling yourself.
Like what more can you want then the sources for all citations in that study, and the study explaining this in length:
During the decision conference participants assessed weights within each cluster of criteria. The criterion within a cluster judged to be associated with the largest swing weight was assigned an arbitrary score of 100. Then, each swing on the remaining criteria in the cluster was judged by the group compared with the 100 score, in terms of a ratio. For example, in the cluster of four criteria under the category physical harm to users, the swing weight for drug-related mortality was judged to be the largest difference of the four, so it was given a weight of 100. The group judged the next largest swing in harm to be in drug-specific mortality, which was 80% as great as for drug-related mortality, so it was given a weight of 80. Thus, the computer multiplied the scores for all the drugs on the drug-related mortality scale by 0·8, with the result that the weighted harm of heroin on this scale became 80 as compared with heroin’s score of 100 on drug-specific mortality. Next, the 100-weighted swings in each cluster were compared with each other, with the most harmful drug on the most harmful criterion to users compared with the most harmful drug on the most harmful criterion to others. The result of assessing these weights was that the units of harm on all scales were equated. A final normalisation preserved the ratios of all weights, but ensured that the weights on the criteria summed to 1·0. The weighting process enabled harm scores to be combined within any grouping simply by adding their weighted scores. Dodgson and colleagues3 provide further guidance on swing weighting. Scores and weights were input to the Hiview computer program, which calculated the weighted scores, provided displays of the results, and enabled sensitivity analyses to be done.
You want the individual data points from all the related studies? All the names and addresses of the people who died and their coroners reports? That’s not how science works, ffs
deleted by creator
I’ve explained in detail and with the actual data where the mortality figures come from. You can’t accept it, because it would mean admitting to how silly you were. Like a teenager who’s just discovered cannabis; “you can’t die of cannabis, this study is fake news!”
Everyone here can see that you’re avoiding answering whether you even logged in to the Lancet to read the study. You didn’t. People here can also see that you’re STILL IGNORING THE THING IVE REPEATED DOZENS OF TIMES; smoking is a popular way of using cannabis and smoking causes cancer.
Anyone reading this will see just how childish you’re being.
It’s okay that you were ignorant and completely wrong. It’s not a sign of weakness, I promise you. However, childish trying to pretend you didn’t make a mistake? Acting like a toddler, because you can’t admit to having lost an argument? That is a sign of weakness.
I’m literally showing you the very source of the statistics. Which you’re just refusing to accept, because presumably you’re incapable of going “oh, my mistake, I was wrong.”
That’s the scientists explaining — in detail — how the data was collected and where from. I also went into the sources of that study. Did you actually log into the Lancet and read the article, or open, see you need an account and go “oh whatever”?
You’ve several times now, asked “do you know the LD50 of cannabis” and “how exactly is cannabis killing people”. Straight up refusing to accept that I’ve explained in detail the difference between drug related and drug specific mortality and how both stats can have things in them without anyone having claimed that a person died of too much cannabis in their system.
Why do you keep ignoring the fact that people SMOKE cannabis and smoking causes a higher mortality rate? I said that before reading the studies, but now that I have done they also explicitly state that, like I KNEW they would.
Both of these quantify deaths from cannabis, but explicitly state the actual LD50 to be unknown, as there’s fewer than three reports of people having died and those can’t be ascertained to be because of cannabis. So they get the LD50 from animals and extrapolate it to humans based on fancy maths. And explicitly state that. Both of them give substances safety ratings. The rating for heroin is 6. Alcohol 10. MDMA 16. The study concludes that they show that MDMA’s dangers have been exaggerated, and it’s inline with cocaine and meth etc. The number for cannabis, you’re asking? They rate it as >1000.
No-one is claiming people are dying of cannabis overdoses, and now that we’re this deep in this thread, there’s no way you’re gonna back on that childish assumption. So I await more bullshit sealioning and excuses despite me linking the methods and sources of all the fucking data from the economist article that you pretend you were too incapable of Googling yourself.
Like what more can you want then the sources for all citations in that study, and the study explaining this in length:
During the decision conference participants assessed weights within each cluster of criteria. The criterion within a cluster judged to be associated with the largest swing weight was assigned an arbitrary score of 100. Then, each swing on the remaining criteria in the cluster was judged by the group compared with the 100 score, in terms of a ratio. For example, in the cluster of four criteria under the category physical harm to users, the swing weight for drug-related mortality was judged to be the largest difference of the four, so it was given a weight of 100. The group judged the next largest swing in harm to be in drug-specific mortality, which was 80% as great as for drug-related mortality, so it was given a weight of 80. Thus, the computer multiplied the scores for all the drugs on the drug-related mortality scale by 0·8, with the result that the weighted harm of heroin on this scale became 80 as compared with heroin’s score of 100 on drug-specific mortality. Next, the 100-weighted swings in each cluster were compared with each other, with the most harmful drug on the most harmful criterion to users compared with the most harmful drug on the most harmful criterion to others. The result of assessing these weights was that the units of harm on all scales were equated. A final normalisation preserved the ratios of all weights, but ensured that the weights on the criteria summed to 1·0. The weighting process enabled harm scores to be combined within any grouping simply by adding their weighted scores. Dodgson and colleagues3 provide further guidance on swing weighting. Scores and weights were input to the Hiview computer program, which calculated the weighted scores, provided displays of the results, and enabled sensitivity analyses to be done.
You want the individual data points from all the related studies? All the names and addresses of the people who died and their coroners reports? That’s not how science works, ffs
Nothing you have pasted, nothing in those studies tell me where the chart got its cannabis mortality figures from or how they calculate them.
So you haven’t read them. And still with this inane sealioning, purposefully ignoring what I keep repeating.
You know smoking is the most popular way of using cannabis. You know smoking causes cancers. You also know these mortality figures have “drug-related” mortality in them, and that is specifically said to be from, among other things, lung cancer.
So stomp your foot all your want but you are wrong and this childish bullshit is making you lose a whole lot of respect you’ve gained on Lemmy.
Methods Study design The analysis was undertaken in a two-stage process. The choice of harm criteria was made during a special meeting in 2009 of the UK Advisory Council on the Misuse of Drugs (ACMD), which was convened for this purpose. At this meeting, from first principles and with the MCDA approach, members identified 16 harm criteria (figure 1). Nine relate to the harms that a drug produces in the individual and seven to the harms to others both in the UK and overseas. These harms are clustered into five subgroups representing physical, psychological, and social harms. The extent of individual harm is shown by the criteria listed as to users, whereas most criteria listed as to others take account indirectly of the numbers of users. An ACMD report explains the process of developing this model.
Fig 1
n June, 2010, a meeting under the auspices of the Independent Scientific Committee on Drugs (ISCD)—a new organisation of drug experts independent of government interference—was convened to develop the MCDA model and assess scores for 20 representative drugs that are relevant to the UK and which span the range of potential harms and extent of use. The expert group was formed from the ISCD expert committee plus two external experts with specialist knowledge of legal highs (webappendix). Their experience was extensive, spanning both personal and social aspects of drug harm, and many had substantial research expertise in addiction. All provided independent advice and no conflicts of interest were declared. The meeting’s facilitator was an independent specialist in decision analysis modelling. He applied methods and techniques that enable groups to work effectively as a team, enhancing their capability to perform,7 thereby improving the accuracy of individual judgments. The group scored each drug on each harm criterion in an open discussion and then assessed the relative importance of the criteria within each cluster and across clusters. They also reviewed the criteria and the definitions developed by the ACMD. This method resulted in a common unit of harm across all the criteria, from which a new analysis of relative drugs harms was achieved. Very slight revisions of the definitions were adopted, and panel 1 shows the final version.
Panel 1
Evaluation criteria and their definitions
Drug-specific mortality
Intrinsic lethality of the drug expressed as ratio of lethal dose and standard dose (for adults)
Drug-related mortality
The extent to which life is shortened by the use of the drug (excludes drug-specific mortality)—eg, road traffic accidents, lung cancers, HIV, suicide
Drug-specific damag…
(I won’t list the rest of the panel because no relation to the matter at hand and you can still look it up yourself, which you’ve been lying about.)
Scoring of the drugs on the criteria
Drugs were scored with points out of 100, with 100 assigned to the most harmful drug on a specific criterion. Zero indicated no harm. Weighting subsequently compares the drugs that scored 100 across all the criteria, thereby expressing the judgment that some drugs scoring 100 are more harmful than others.
In scaling of the drugs, care is needed to ensure that each successive point on the scale represents equal increments of harm. Thus, if a drug is scored at 50, then it should be half as harmful as the drug that scored 100. Because zero represents no harm, this scale can be regarded as a ratio scale, which helps with interpretation of weighted averages of several scales. The group scored the drugs on all the criteria during the decision conference. Consistency checking is an essential part of proper scoring, since it helps to minimise bias in the scores and encourages realism in scoring. Even more important is the discussion of the group, since scores are often changed from those originally suggested as participants share their different experiences and revise their views. Both during scoring and after all drugs have been scored on a criterion, it is important to look at the relativities of the scores to see whether there are any obvious discrepancies.
Weighting of the criteria
Some criteria are more important expressions of harm than are others. More precision is needed, within the context of MCDA, to enable the assessment of weights on the criteria. To ensure that assessed weights are meaningful, the concept of swing weighting is applied. The purpose of weighting in MCDA is to ensure that the units of harm on the different preference scales are equivalent, thus enabling weighted scores to be compared and combined across the criteria. Weights are, essentially, scale factors.
MCDA distinguishes between facts and value judgments about the facts. On the one hand, harm expresses a level of damage. Value, on the other hand, indicates how much that level of damage matters in a particular context. Because context can affect assessments of value, one set of criterion weights for a particular context might not be satisfactory for decision making in another context. It follows then, that two stages have to be considered. First, the added harm going from no harm to the level of harm represented by a score of 100 should be considered—ie, a straightforward assessment of a difference in harm. The next step is to think about how much that difference in harm matters in a specific context. The question posed to the group in comparing the swing in harm from 0 to 100 on one scale with the swing from 0 to 100 on another scale was: “How big is the difference in harm and how much do you care about that difference?”
During the decision conference participants assessed weights within each cluster of criteria. The criterion within a cluster judged to be associated with the largest swing weight was assigned an arbitrary score of 100. Then, each swing on the remaining criteria in the cluster was judged by the group compared with the 100 score, in terms of a ratio. For example, in the cluster of four criteria under the category physical harm to users, the swing weight for drug-related mortality was judged to be the largest difference of the four, so it was given a weight of 100. The group judged the next largest swing in harm to be in drug-specific mortality, which was 80% as great as for drug-related mortality, so it was given a weight of 80. Thus, the computer multiplied the scores for all the drugs on the drug-related mortality scale by 0·8, with the result that the weighted harm of heroin on this scale became 80 as compared with heroin’s score of 100 on drug-specific mortality. Next, the 100-weighted swings in each cluster were compared with each other, with the most harmful drug on the most harmful criterion to users compared with the most harmful drug on the most harmful criterion to others. The result of assessing these weights was that the units of harm on all scales were equated. A final normalisation preserved the ratios of all weights, but ensured that the weights on the criteria summed to 1·0. The weighting process enabled harm scores to be combined within any grouping simply by adding their weighted scores. Dodgson and colleagues3 provide further guidance on swing weighting. Scores and weights were input to the Hiview computer program, which calculated the weighted scores, provided displays of the results, and enabled sensitivity analyses to be done.
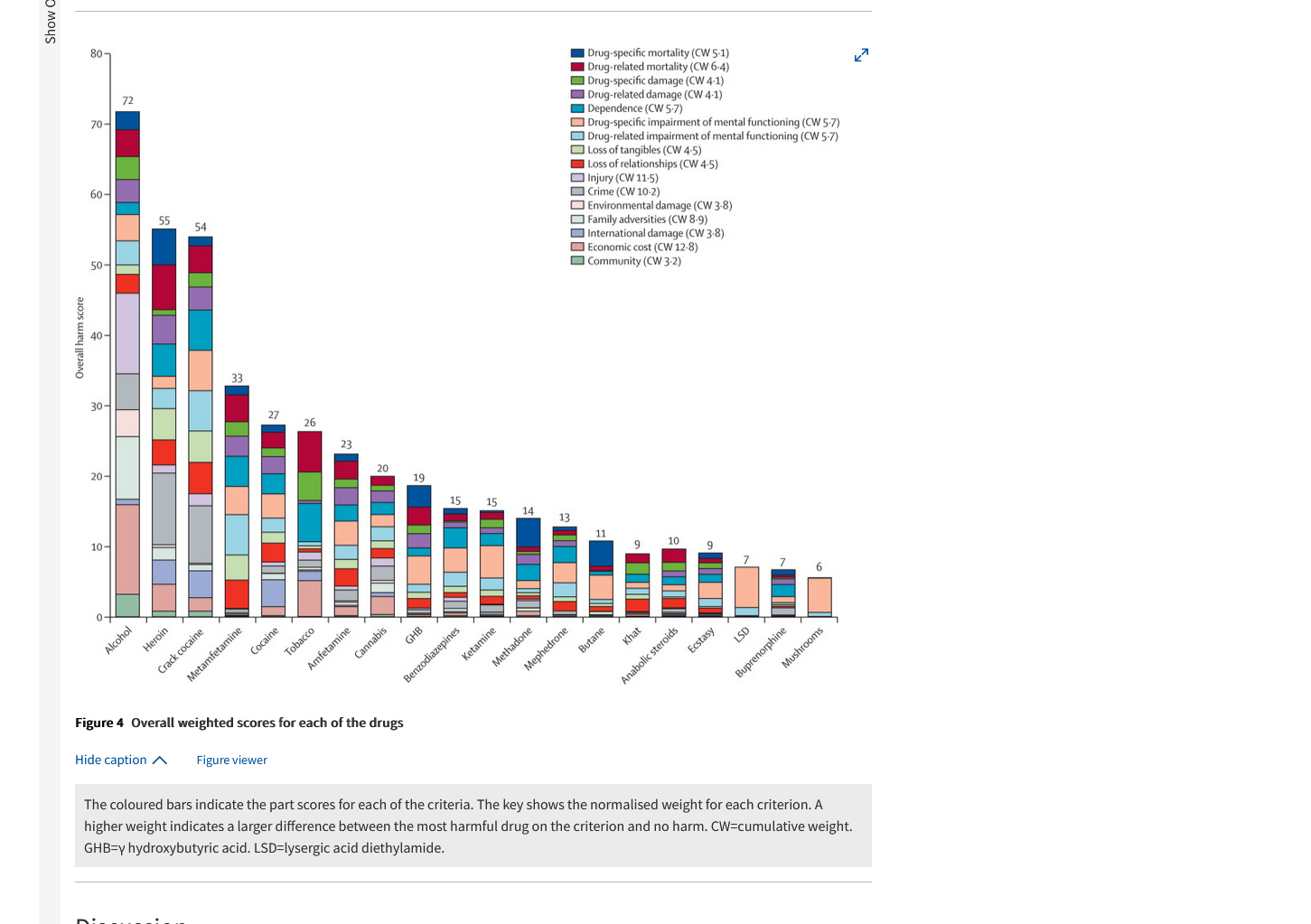
Figure 4 shows the contributions that the part scores make on each criterion to the total score of each drug. Alcohol, with an overall score of 72, was judged to be most harmful, followed by heroin at 55, then crack cocaine with a score of 54. Only eight drugs scored, overall, 20 points or more. Drug-specific mortality was a substantial contributor to five of the drugs (alcohol, heroin, γ hydroxybutyric acid [GHB], methadone, and butane), whereas economic cost contributed heavily to alcohol, heroin, tobacco, and cannabis.
We also investigated drug-specific mortality estimates in studies of human beings.13 These estimates show a strong correlation with the group input scores: the mean fatality statistics from 2003 to 2007 for five substances (heroin, cocaine, amfetamines, MDMA/ecstasy, and cannabis) show correlations with the ISCD lethality scores of 0·98 and 0·99, for which the substances recorded on the death certificates were among other mentions or sole mentions, respectively.
So just like I’ve said FROM THE START, the mortality comes from drug-related disease, like lung cancer, and drug-specific mortality comes from dying in a car crash with the coroner reporting cannabis AMONG other substances, which will still make it count towards the stat, while not having had an effect on the crash compared to the others. But no. You sit there claiming that I haven’t understood and that these studies somehow claim that people are dying of cannabis-overdoses. Which you’ve asked explicitly several times over, despite me trying to explain this to you in the simplest way possible.
My god, more excuses.
No need to reply to my one sentence comment pointing out the same problem were arguing here. Just answer the comment above yours.
It is, yes.
Drug-specific mortality and drug-related mortality are two different things.
Nutt, who is apparently aptly named, because he’s apparently just making shit up.
You’re being serious? Discrediting all of his science, because he’s probably bias? Not childish at all.
I read your links. You clearly did not.
No you didn’t.
Did you read the full text from the Lancet? (It’s free but requires logging in.)
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)61462-6/fulltext#box1
You started this protest by protesting the “mortality” bit of the chart. (Which, admittedly, I had forgotten about.) We then started arguing over it, you going on about people claiming there are arguments of “cannabis killing people” and asking me if I “know the LD50 of cannabis”. I replied by saying that I know about studies like this, and I understand that the mortality figures also come from drug-related diseases, like lung cancer if you’ve smoked the substance of your choice. You ignored that bit, and are still ignoring it.
From that link:
Drug-specific mortality Intrinsic lethality of the drug expressed as ratio of lethal dose and standard dose (for adults) Drug-related mortality >The extent to which life is shortened by the use of the drug (excludes drug-specific mortality)—eg, road traffic accidents, lung cancers, HIV, suicide
Road traffic accidents and lung cancers? Just like I said way back. That yes, the mortality stat is sus to an extent, because of the mechanism of say, a drunk driver killing themselves, then having blood taken, it having cannabis, and that being attributed to cannabis mortality. However, the other part which is more objectively reasonable is the lung cancer bit. Why? Because it’s very popular to SMOKE cannabis and smoking anything causes cancer.
I do not have access to the individual datapoints of their study. They’ve used sophisticated software to analyse it. Do you think you’d analyse the data better?
My point has been, all the time, that while the data for mortality probably isn’t accurate, we can say for certain that some, probably most of it, is due to the increased mortality from smoking. Like I said, if everyone just ate it, the mortality should be zero, and if we knew everyone took edibles and never smoked, and if there still was a wide mortality rate in a chart like that, then we could say it was wholly suspect.
See if you had actually opened the full study on the Lancet, you’d have seen that more accurate chart. Almost as if you didn’t and are just somewhat childishly trying to win this debate, even though I consider it a conversation and thus there are no winners or losers. I’m not arguing anything. I’m saying I know that most of the mortality is due to smoking reducing lifespans and a lot of cannabis being smoked. I too smoke. It’s unhealthy. I’ve tried changing to vapes several times, but it’s just not as good. A dab pen would be. Maybe even just an electric nail to my bong. But then making my own dab feels like a waste as smoking bud just makes it last longer.
You can’t torture the money away from most billionaires. Someone who has most of their wealth in Bitcoin theoretically could have that happen to them.
And after stealing the money, there’s not that much chance of getting caught, unlike if you just tried putting billions into your regular ass bank account.


Oh well. Any votes destroyed is bad.